Cleft Lip and Cleft Palate
What is a cleft lip/cleft palate?
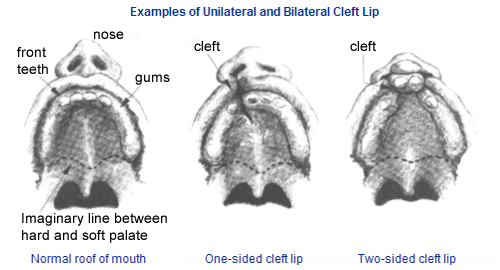
A cleft lip is a separation of the two sides of the lip. Sometimes this includes the bone of the upper jaw. A cleft palate is an opening in the roof of the mouth in which the two sides of the palate did not join together. Cleft lips and palates can be unilateral ( a cleft on one side) or bilateral (a cleft on both sides). Cleft lips are called ‘complete’ clefts when the opening extends through the nose. Cleft Palates may also be called ‘complete’ (extending through the entire roof of the mouth) or ‘incomplete’.
Why did this happen?
Around the 6th week of pregnancy, the parts of the lip usually join together. The palate should close around the 11th week of pregnancy. When for some reason this process does not occur, the result is a cleft lip and or cleft palate. There may be genetic or environmental reasons for the clefts. A genetic link is suspected when other family members have cleft. Some clefts can be linked to certain syndromes or clusters of health problems. Most cleft lips with or without cleft palate are isolated clefts (no other medical conditions). Since clefts occur so early in pregnancy, it is often difficult to identify possible exposures that are linked to clefts. It is a good idea to have a genetic evaluation to identify possible causes.
Here are some statistics to help you understand the frequency of clefts: A ‘Cleft Lip with or without a Cleft Palate’, or a ‘Cleft Palate only’ are two of the most common birth defects.
Clefts occur in 1 in 700 newborns.
Clefts occur more often in Asian and Native American populations; least often in African Americans.
Cleft Lips and Palates occur more in males than females
Cleft Palates alone occur more often in females than males; unilateral cleft lip is more common that bilateral. Left sided clefts are more common than right sided.
There is a 2-5% chance that once parents have one child with a cleft that they will have another child born with a cleft. The risk of having a child with a cleft will increase if there are other family members with clefts.
What is the treatment of cleft lip/cleft palate?
Almost all children born with clefts will have surgery during their first year of life.
The lip is repaired at 3-4 months of age and the palate is repaired between 9-12 months. The actual timing depends on the child’s growth and on the pre-surgical treatment plan. Non-surgical treatment, called Pre-surgical Nasal Alveolar Molding (PNAM) requires the use of a dental appliance made to fit the roof of your infant’s mouth. This pre-surgical molding influences the growth of the tissue and reduces the size of the opening so that the first surgery gets better results. This process should begin during the first weeks of life. (Read more about Molding).Secondary repair- if needed- occurs at approximately 4-6 years. An Alveolar bone graft may be necessary to fill the gap (cleft) in the gum where the teeth come in and is repaired at 8-10 years.
Final lip and/or nose revisions are done at 14-16 years if necessary.
It is important to note that every child is different. Some children may require more surgeries than others, while others may require fewer. This all depends on the severity of the cleft, the absence of tissue or how the child heals after surgery is completed.
Cleft Lip Repair:
This first surgery is generally done between 3-6 months of age. Timing will depend on your infant’s weight and general health as well as the progress of any pre-surgical treatment that is part of your treatment plan. Lip repair is generally done as a day surgery procedure and you will take your baby home the same day. After the lip is repaired you will continue to use the same feeding method (nipple or tube) until you wean your infant from the nipple to a cup in preparation for the palate repair. If your baby used a pacifier or used a dental appliance as a pacifier, it may take a few days after the surgery to stop missing it.
Cleft Palate Repair:
Most cleft palates are repaired between 9-12 months. This is done before speech develops so that your child does not develop speech habits that will difficult to understand. You should make an appointment to see the surgeon when your baby is about 7 ½ months old. He will advise you when he thinks your child will be ready for this surgery. If it is possible, you should wean your child to a sippy cup before this surgery because bottle feeding is prohibited for two weeks after the palate repair.
Prior to scheduling surgery, you should have fluid and the team’s Pediatric Otolaryngology or ENT (Ear, Nose and Throat )doctor examine your child. Ear infections are common with cleft palates and frequent ear infections can cause hearing loss. If the ENT doctor recommends tubes be placed to help keep the ears open, it may be possible to do both procedures at once.
There are several different ways to repair a cleft palate. Tissue in the palate will be detached and rearranged to close the cleft. The muscles of the soft palate are also re-positioned to aid speech. The surgeon will determine which method will work best for your child during surgery.
Cleft Palate repair is a longer procedure than repair of the lip and requires a 2 to 3 day hospital stay. This is because post operative swelling can block your child’s airway and so we can insure your child gets enough fluids until he or she begins drinking after surgery.
POST OP INSTRUCTIONS:
- Most children have a tongue stitch during palate surgery to prevent any breathing problem afterwards. This stitch will be removed the next morning.
- Restraints called “No No’s” will be placed on your child’s arms to prevent bending the arm close enough to touch the tender area of the mouth with fingers or toys. These restraints can be removed under CLOSE supervision for bathing and exercise. The restraints should be kept on for one week (or two if your child puts things in his mouth).
- Your child may be fussy and sore but pain medication will be given if needed. After the prescription pain medication is finished or no longer necessary, pain can be managed with children’s Tylenol or children’s Motrin/Advil.
- We encourage you to wean your child to a sippy cup before surgery. However, if the child is still taking a nipple, you will need to use a rubber catheter and a syringe to deliver liquids between the jaw and cheek (avoiding the palate). Do NOT put anything into the mouth to cause injury for 14 days after surgery. Do not use utensils or straws. Your child can have the same liquids as before surgery. The foods should be soft and almost fluid. You may need to add water or run the food through a blender to make it easy to eat. Jello cubes are a good source of fluid.
- The palate takes about three weeks to heal. A scab (eschar) inside the mouth will appear white. The stitches will take
3-4 weeks to completely disappear. Swelling may take longer to completely disappear. - The baby’s palate will be somewhat stiff after surgery. It can take three to six months until it is moving adequately.
- Be sure to call to make an appointment to see the doctor as written in your discharge instructions. This is usually 7-10 days after discharge. Call as soon as possible to make a post op appointment.
- If there are any medical problems, please call the doctor’s office at any time (832)325-7234. If you have non medical questions contact the Coordinator at 713-500-7302.
Feeding:
Children with cleft of the lip and palate may have difficulty sucking and swallowing. This is related to the lack of appropriate structure to suck efficiently from the bottle or the breast. This puts them at risk for failure to gain weight and even weight loss.
There are several types of bottles and nipples that are made for feeding a baby born with a cleft. Most babies with a cleft of the lip and palate will have difficulty breast feeding or feeding with regular bottles. For some babies finding the right method may just be trial and error. Most babies will learn to feed with one of the feeding systems available.
To help with feeding, the baby should be held in an upright position and burped frequently. Some infants benefit from a dental appliance fitted by a dental specialist. It provides a hard surface against which to press the nipple during feeding.
The general feeding guidelines for parents is that the infant should take the required feed in about 30 minutes. If it takes much longer than 45 minutes to take the full amount, the child may be working too hard and not getting enough food to grow. If this occurs another feeding method should be tried. We encourage a consultation with the Team feeding specialist.
Speech Issues:
Children with cleft lip and cleft palates may have more difficulty being understood than other children. Children who have a cleft of the palate only or a cleft of the lip and palate are at risk for communication problems even when the palate is repaired during the first year of life. Sometimes the soft palate lacks adequate structure, length, and mobility for normal speech to develop. Some children learn incorrect patterns of articulation to compensate for structural differences and their inability to produce pressure consonants.
Children with cleft lip and palate are also at risk for more ear infections and fluctuating hearing places them at risk for problems with learning communication.
Most children with cleft lip and/or palate develop normal speech once their palate is closed. According to the Cleft Palate Foundation 20-25% will need further surgery, speech therapy or a prosthetic speech aid to improve their speech.
We recommend children born with clefts be referred for Early Childhood Intervention (ECI) programs. The ECI program in Texas includes speech pathologists and is offered to children up to age 3 years of age. Early referral to ECI may be appropriate for babies with feeding problems or other developmental delays. Once your child is beginning to babble or if speech is delayed, you should request ECI services. There are also speech pathologists in private practice and in hospitals who are experienced in working with children with cleft palates. It may be helpful to supplement the treatments provided by ECI or the public school system if communication problems persist.
Children with cleft lip/palate will need the services of a Speech/Language Pathologist from early infancy throughout their childhood years. Some will need occasional evaluation and monitoring while others will need help with oral motor development and feeding as well as yearly evaluations and ongoing speech and language therapy.
The role of the speech pathologist in children who have cleft lip/palate:
- Assessment of oral motor functioning, feeding and swallowing.
- Assessment of communication.
- Providing parent education and support
- Improving infant’s or child’s oral motor functioning and feeding patterns.
- Providing ongoing speech and language therapy when needed.
Assessment of a child with cleft lip/palate includes the following:
- Case history
- Review of medical record
- Review of hearing status and referral if necessary
- Swallowing/feeding evaluation
- Instrumental diagnostic procedures (modified barium swallowing study, video fluoroscopy of palatal motion and nasoendoscopy).
- Oral motor evaluation, including: symmetry, oral sensation, strength, and range of motion and oral mobility.
- Communication assessment, including: articulation, receptive and expressive language, voice, and resonance.
Many children with cleft lip and/or palate develop normal speech once their palate is closed. According to the Cleft Palate Foundation 20% will need further surgery, speech therapy or a prosthetic speech aid to improve their speech. The speech of these children may be difficult to understand because of one or all of the following communication problems:
- Language delay – many cleft palate children are slow to begin to speak, to develop vocabulary and to put sentences together.
- Articulation problems- these children have difficulty pronouncing sounds correctly and frequently have developed incorrect patterns to compensate for their structural differences. Speech therapy is helpful in teaching proper placement of the lips and tongue for speech sounds and to help parents learn techniques to help their children speak well.
- Hypernasality – The speech of many cleft palate children sounds nasal (referring to the nose) rather than oral (referring to the mouth). Only three speech sounds should be produced through the nose. These are ‘M’ as in “Mama”; ‘N’ as in “No”; and ‘ng’ as in “ring”. Some cleft palate children have nasal sounding speech most of the time. Children with severe hypernasality may need additional surgery as well as speech therapy to improve their speech enough to be understood by others. Oral motor stimulation can be helpful in improving feeding, articulation and in decreasing hypernasality.
- Voice problems: occasionally children with cleft palate may develop vocal nodules secondary to vocal abuse that occurs when they increase their volume in an effort to make themselves heard and understood.
A competent speech language pathologist should treat all children with cleft lip/palate. This person should have Master’s Degree, a State license to practice, and a certificate of clinical competence conferred by the American Speech Language and Hearing Association. It is also helpful if the speech pathologist has some experience working with children who have cleft lip and cleft palate.
The first communication assessment should be done shortly after birth. This is to see if feeding is going well. Oral motor stimulation techniques may also be taught to the parent. Follow up visits may be helpful. The second evaluation should occur at 12-18 months with yearly evaluations needed during the first 7 years of life. Speech and language therapy will be recommended when appropriate. A few will need to continue with yearly evaluation through high school in order to monitor need for intervention after orthodontic changes.
Pre-surgical Nasal Alveolar Molding:
Infants born with clefts of the primary and secondary palate might be candidates for molding treatment prior to any surgical repairs if recommended by the Plastic Surgeon. Pre-Surgical Nasal Alveolar Molding (PNAM) is a method of treatment that reshapes the infant’s nose without surgery through the use of a custom made orthopedic denture plate.
Molding should begin within the first few days or weeks of life. The Pediatric Dentist takes a dental impression of your baby’s mouth and fabricates a appliance that is unique to your baby’s mouth. The appliance is a hard piece of plastic that fits to the roof of the mouth. Once your baby gets used to wearing it, nasal prongs are added to lift the nostril(s). At the same time, tape is used to move and reshape the tissue segments. The molding device is worn 24 hours a day and is removed only for cleaning. Molding is a continuous process that requires weekly visits to the pediatric dentist. At each visit the pediatric dentist will adjust the shape of the appliance and re-position the nasal prongs. She will also make changes in the taping instructions to achieve proper alignment of the nose and lips. This slow movement continues until the pediatric dentist is satisfied with the position of the tissue and cartilage and consults with the Plastic Surgeon. If both are satisfied that the optimum position has been attained, the lip is surgically repaired. Pre-Surgical Nasoalveolar Molding is an outpatient treatment that lasts from 3-6 months depending upon the amount of movement needed.
Pre-surgical Nasoalveolar Molding can rotate the pre-maxilla, straighten the columella, lengthen the prolabium, lift the alar (nostril), and aligns the alveolar ridge (gum).
Nasal Alveolar Molding Appliance
Parents are responsible for the day to day compliance with the molding instructions. It is important that you understand the commitment necessary to follow the molding protocol established by the pediatric dentist. It is this partnership between the parents, dentist, and plastic surgeon that achieves the desired outcomes of Pre-surgical Nasoalveolar Molding.

It is important to know that molding can reduce the size and number of surgeries for many patients. However, it is likely that orthodontic treatment will and/or bone grafting (to close any remaining gap in the alveolar ridge) may be necessary as your child grows.