Craniosynostosis
The surgical team at Children’s Memorial Hermann Hospital includes a pediatric neurosurgeon and craniofacial surgeon as well as a specialized anesthesiologist. The neurosurgeon works on the skull and the craniofacial surgeon on the face. With both areas being closely related the combined approach offers the best possible results with the highest level of safety.
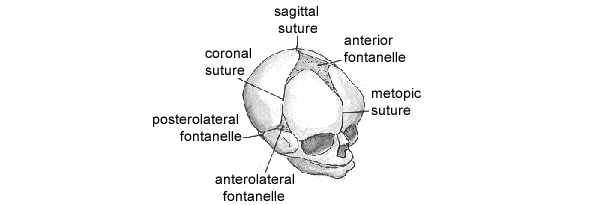
The skull of an infant is made up of free-floating bones separated by fibers called sutures. This arrangement allows the infant’s head to pass through the birth canal and also enables the skull to grow with the brain in early infancy.
Premature fusing of the sutures is called craniosynostosis, which restricts skull growth. The cause of this premature fusion is unknown. Simply put, synostosis is the union of two or more bones to form a single bone. Children born with craniosynostosis may have increased pressure on the brain and vision problems. They may also have low self-esteem and behavioral problems due to an abnormal head shape. Long-term studies demonstrate that in addition to correcting functional problems associated with craniosynostosis, reconstructive surgery has a positive effect on the child’s self image and the ability to get along with his or her peers.
Diagram of skull, showing location of fontanelles and sutures
How is craniosynostosis diagnosed?
Diagnosis begins with an examination by the pediatric neurosurgeon and the craniofaciaI surgeon. A distorted head at birth does not always result from craniosynostosis. The initial history involves questions about abnormal fetal position and neck tightness, which can cause positional deformities which do not require surgery. The physical examination involves carefully feeling the skull for suture ridges and soft spots, or fontanelles, and checking for neck position and other deformities. Measurements are taken of the child’s face and head. Computerized tomography, a series of photographic images of the brain, is ordered since they provide the most reliable method of diagnosing early suture fusion. These are needed when planning the surgical correction.
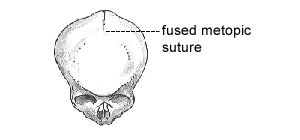 |
Diagram of metopic synostosis, showing effect of premature closure of the metopic suture. |
What is Metopic Synostosis?
The metopic suture begins at the nose and continues upward to meet the sagittal suture. Metopic craniosynostosis results in a narrow, triangular forehead with pinching of the temples laterally. Treatment involves releasing the suture and expanding and rounding out the upper face, forehead and skull.
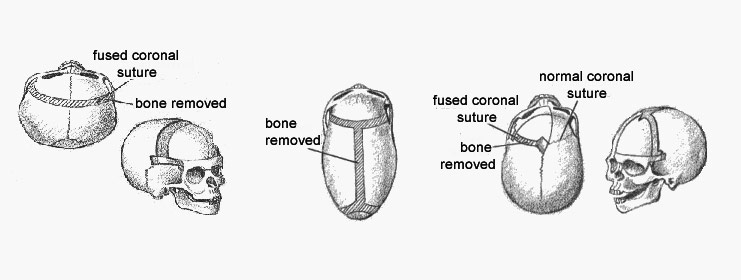
What is coronal synostosis?
The coronal sutures begin at the ear and continue superiorly to the top of the skull to meet the sagittal suture. One or both sutures may be involved. When one suture is fused, the forehead on that side is flattened and swept back with the eye and its socket. When both sides are fused, the head is short and wide with bulging of the eyes and bulging of the skull around the ears. The surgical correction depends on whether one or both sutures are involved. When one suture is fused, it is removed and the forehead and brow reshaped and brought forward to match the other side. In addition, the cheek is also brought forward to reposition the eye socket. When both sutures are fused, they are both removed and the skull is narrowed and lengthened. In addition, both cheekbones are brought forward to reposition the eye socket.
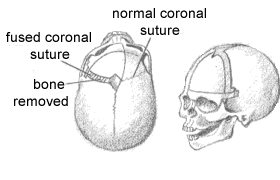 |
Diagram of left sided coronal synostosis in which one coronal suture had closed prematurely and needed repair |
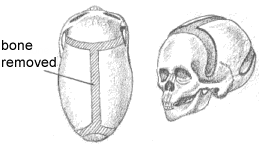 |
Diagram of bilateral coronal synostosis in which both coronal sutures had closed prematurely and needed repair |
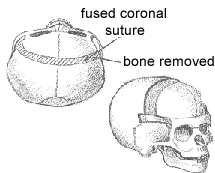 |
Diagram of sagittal synostosis in which the sagittal suture had fused prematurely and needed repair |
What is sagittal synostosis?
The sagittal suture runs from a spot at the front of the head to the back of the skull. Fusion of the suture results in a long, narrow skull with or without bulging of both the front and back of the head. Surgery of sagittal craniosynostosis involves removing the suture and widening the skull by opening up the coronal and lambdoid sutures on both sides of the head. Sometimes bone grafts are placed to keep the out-fractured bones apart.
What is multiple suture synostosis?
When all the sutures are fused, the children are operated on as soon as possible. The sutures are all released and the bones are all repositioned to allow for normal brain growth and to relieve the pressure on the eyes and brain.
When should surgery be done?
For some children, the ideal timing for surgery is prior to 3 months of age when a less- invasive, microscopic procedure can be used that results in a smaller incision, less blood loss and a shorter hospital stay than the traditional corrective surgery. Early surgical intervention is advised because the bones of the skull are easy to work with at this age, and the covering of the brain, known as the dura, can make bone on its own. Moreover, the growing brain can continue to reshape the skull and face after the surgery. Although surgery is done early in life, there is no upper age limit to surgery. Usually one surgery is required to correct children with simple craniosynostosis, although some may need minor alterations at 4-5 years of age. Children with craniofacial syndromes as well as craniosynostosis require several surgeries on the skull to achieve a normal shape.
How is the child cared for after surgery?
After surgery, the child remains in the Pediatric Intensive Care Unit for 1-3 days, depending on the surgery. Swelling is most noticeable 2-3 days after surgery and takes several weeks to completely resolve. In a patient with significant facial swelling, the breathing tube is left in place to protect the air passage. This remains until the swelling improves and the patient can breathe on his or her own.
The child is usually eating and drinking within several days after surgery. Once the bandage is removed, the scalp is cleaned to remove all crusts. Absorbable sutures are used, which do not require removal. When the child is discharged, parents need to be watchful for any redness or drainage around the suture line, which may be a sign of infection.
Before and after patient photographs at 1 and 6 months (Sagittal Synostosis)


Before and after patient photographs at 1 and 6 months (Sagittal Synostosis)

