STAT Interventional Radiology Consult (“IR STAT Trauma”) Clinical Practice Policy
Original Date: 02/2017 | Last Review Date: 04/2025
Purpose: To decrease Interventional Radiology response time for critically injured patients.
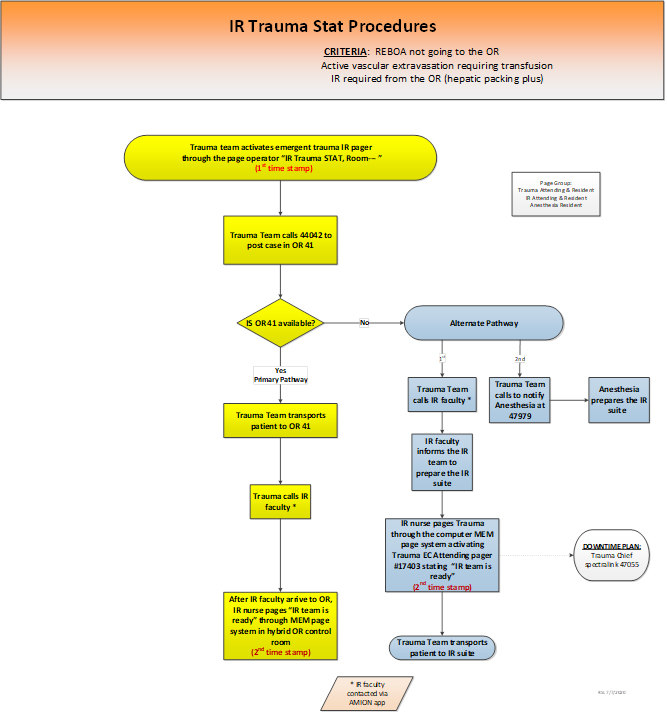
Indications for Activation of “IR STAT Trauma”
- Patient with REBOA not going to the OR for surgical hemorrhage control
- Active vascular extravasation requiring transfusion
- IR required from the OR (e.g hepatic or pelvic packing)
Location of IR STAT Trauma procedures
IR STAT Trauma patients will preferentially be treated in the hybrid operating room (OR 41) with both Interventional Radiology (IR) and Trauma services. OR and IR nursing teams will provide care in the hybrid OR suite. The IR suite will be used if the hybrid OR is not immediately available.
Process for IR STAT Trauma in hybrid OR
- When the trauma attending identifies a patient requiring emergent hemorrhage control from interventional radiology (IR), the trauma team activates the trauma IR pager through the page operator (4-3333) by requesting “IR STAT Trauma to OR 41.”
The decision to activate the IR STAT Trauma pager must be made by the trauma attending. - The trauma team calls the OR front desk (4-4042) to post the emergent case in OR 41. Post for STAT IR angiography/embolization (specify location if known – pelvis, spleen, liver, etc) under trauma faculty name.
- The trauma team calls the anesthesia team (4-7979) to notify of IR STAT activation.
- The trauma team and ED nursing staff transports the patient to OR 41.
- The trauma team (faculty if available) calls the IR faculty* to specify location of procedure in OR 41 and location of bleeding.
- All IR team members, including faculty, resident, tech, and nurse, will receive a page stating “STAT Trauma IR” and immediately report to the hybrid OR without causing delay.
- The IR RN places verbal order under the trauma attending for IR Consult Order.
- The IR team places the procedure on the snapboard.
- When the IR team (including faculty) arrive to the hybrid OR, the trauma team will receive a page stating “IR team is ready”.
Process for IR STAT Trauma in IR suite
- When the trauma attending identifies a patient requiring emergent hemorrhage control from interventional radiology (IR), the trauma team activates the trauma IR pager through the page operator (4-3333) by requesting “IR STAT Trauma to IR Angio Suite.”
The decision to activate the IR STAT Trauma pager must be made by the trauma attending. - The trauma team (faculty if available) calls the IR faculty* to specify location of procedure in the IR suite and location of bleeding.
- The trauma team places an IR Consult Order in Epic.
- The IR team places the procedure on the snapboard.
- After activating IR STAT Trauma, the trauma team will notify Anesthesia (4-7979) of the need for assistance in IR.
- The trauma team and ED nursing staff transport the patient to the IR suite.
- All IR team members, including faculty, resident, tech, and nurse, will receive a page stating “STAT Trauma IR” and immediately report to the IR suite without causing delay.
- When the IR team is ready (including faculty in the IR suite), the trauma team will receive a page stating “IR team is ready”
Background
The American College of Surgeons Committee on Trauma (ACS-COT) now requires an experienced Interventional radiologist to be available within 30 minutes to perform interventional procedures for level 1 and level 2 trauma centers. The IR STAT Trauma policy was created in 2017 to comply with this new guideline to maintain our level 1 trauma center verification.
The trauma service has activated IR STAT Trauma on 107 patients since March 2017 with a 58% therapeutic embolization rate and 72% survival rate despite elevated injury severity scores (median ISS 34 for all, ISS 34 for survivors, and ISS 43 for deaths).
Location of Hemorrhage and Outcome Data
| Number of patients (n, %) | Therapeutic embolization (%) | Survival rate (%) | |
|---|---|---|---|
| Pelvis | 61 (57%) | 61% | 77% |
| Liver | 29 (27%) | 45% | 62% |
| Spleen | 6 (5.6%) | 100% | 100% |
| Other location* | 11 (10%) | 55% | 64% |
*other locations include renal and mesenteric injuries
Indication for IR STAT Trauma Activation by Location of Hemorrhage
| Number of patients (n, %) | Survival rate (%) | Pelvis | Liver | Spleen | |
|---|---|---|---|---|---|
| Active vascular extravasation requiring transfusion | 61 (57%) | 77% | 64% | 45% | 67% |
| Need for IR from OR | 25 (23%) | 64% | 18% | 38% | 0% |
| REBOA | 8 (7.5%) | 50% | 13% | 0% | 0% |
| MD discretion | 7 (6.5%) | 86% | 3% | 7% | 16.5% |
| Other | 6 (5.6%) | 83% | 1% | 10% | 16.5% |
| Number | % Therapeutic | |
|---|---|---|
| Indication: | ||
| Active vascular extravasation requiring transfusion | 61 | 63% |
| REBOA | 8 | 50% |
| MD discretion | 7 | 33% |
| IR from OR/IR in OR | 25 | 52% |
| Other | 6 | 67% |
| Liver: | ||
| Active vascular extravasation requiring transfusion | 13 | 62% |
| MD Discretion | 2 | 0% |
| IR from OR/IR in OR | 11 | 36% |
| Other | 3 | 33% |
*IR faculty can be reached through the page operator or the Amion app (type: “houston ir” in the search box). The on-call IR attending is listed under “second call”. Please use the cell phone number and not the pager to communicate with the IR faculty.