Late Entry, Addendum, Amendment, or Attestation?

Pexels: Min An
Understanding Intent, Compliance Boundaries, and Audit Risk
Accurate medical documentation must be contemporaneous, complete, and truthful. When documentation is modified after the fact, CMS and professional societies recognize limited, well‑defined mechanisms to correct or clarify the medical record. However, post‑service documentation carries heightened audit risk, especially when used to support payment after a claim has already been submitted.
Late Entry
Definition
A late entry adds omitted information that the provider knew and performed at the time of service. The provider must have total recall of the event and must clearly label, date with the current date, time, and sign the entry. Providers may not back‑date late entries.
Intent
✅ Clarify or complete missing factual documentation
❌ Not intended to recreate memory or justify services retrospectively
Compliance Focus
- Clarification of what actually occurred
- Transparency in timing and authorship
High‑Risk Uses
- Added after claim submission to support medical necessity
- Added weeks or months later without clear linkage to the original note
Audit Risk Signals
- Appears only after an ADR, CERT, TPE, or appeal
- Adds diagnoses, time, or decision‑making not referenced elsewhere
- Used to upgrade E/M level or justify services denied initially
Addendum
Definition
An addendum provides new or additional information that was not available at the time of the original entry, such as diagnostic results received later. The addendum must reference the original note, be clearly labeled, dated, timed, and signed.
✅ Supplement documentation with new clinical data
❌ Not to correct omissions or alter clinical reasoning retroactively
Compliance Focus
- Clarifying evolving clinical information
- Preserving the integrity of the original record
High‑Risk Uses
- Addenda used to insert medical decision‑making after billing
- Addenda written in response to denial language
Audit Risk Signals
- Addendum materially changes acuity or complexity
- Appears tailored to coverage criteria rather than patient care
- No indication the information was unavailable initially
Amendment
Definition
An amendment is a formal modification to the medical record, often initiated due to identified inaccuracies or patient requests under HIPAA. Amendments must preserve the original content, identify what was changed, why, by whom, and when.
Intent
✅ Correct inaccuracies while maintaining transparency
❌ Not to revise clinical judgment after outcomes are known
Compliance Focus
- Integrity and traceability of the record
- Compliance with HIPAA and CMS recordkeeping principles
High‑Risk Uses
- Altering clinical facts after adverse events
- Amendments tied directly to billing disputes or litigation
Audit Risk Signals
- Original content obscured or deleted
- No rationale for amendment
- Timing suggests payment motivation
Attestation
Definition
An attestation is a provider’s statement confirming presence, participation, supervision, or authorship—commonly used for teaching physician requirements, split/shared visits, or resident supervision. Attestations do not create new clinical facts.
Intent
✅ Confirm compliance with regulatory participation requirements
❌ Not to add missing clinical documentation
Compliance Focus
- Regulatory confirmation (e.g., “I was present and participated…”)
- Clear linkage to existing documentation
High‑Risk Uses
- Attempting to substitute for missing history, exam, or MDM
- Generic or templated attestations appended post‑billing
Audit Risk Signals
- Attestation conflicts with underlying note
- No corroborating documentation of provider involvement
- Used to justify billing level or service independently
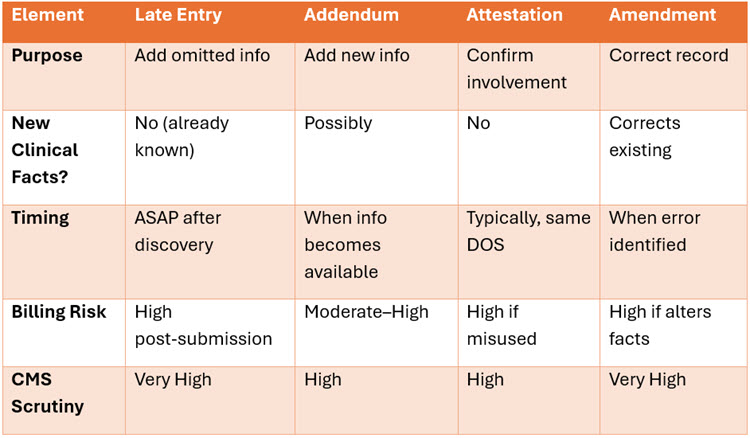
Side-by-Side Comparison
This table distinguishes at-a-glance the differences in each type of entry.
Texas Medicaid & Novitas JH
- Texas Medicaid follows CMS recordkeeping principles and expects complete, contemporaneous documentation at time of service. Post‑payment record changes are heavily scrutinized during appeals and recoupments.
- Novitas JH explicitly states that entries not meeting amendment principles will not be considered during medical review.
Final Key Compliance Takeaways
✅ Documentation tools exist to clarify, not manufacture, clinical support.
❌ Any post‑billing documentation used to justify payment is presumed high‑risk.
✅ Transparency, timing, and traceability are non‑negotiable.
❌ If it changes medical necessity, acuity, or coding justification, expect scrutiny.
Authoritative Resources
- Noridian – Documentation Guidelines for Amended Medical Records
- CMS Medicare Program Integrity Manual, Pub. 100‑08, Ch. 3 §3.3.2.5
[cms.gov] - Novitas JH – Amendments, Corrections & Delayed Entries
[novitas-so…utions.com] - AHIMA – Amendments in the Electronic Health Record
[ahima.org] - AAPC – Making Amendments, Corrections, and Delayed Entries
[aapc.com]