Post-Traumatic Seizure Prophylaxis in Patients with Traumatic Brain Injury Clinical Practice Guideline
Original Date: 08/2005 | Last Review Date: 07/2024
Purpose: To standardize the delivery of post-traumatic seizure prophylaxis in patients with traumatic brain injury.
Overview:
Traumatic Brain Injury (TBI) is an anatomical and functional insult to the brain. TBI-induced cerebral injury is a combination of physical, cellular, and vascular insults. Post-traumatic seizure (PTS) is a known sequela of TBI and can be categorized as immediate (occurring within 24 hours of injury), early (within 24 hours to seven days after injury), or late (occurring greater than seven days after injury). Early PTS increases the risk of late PTS (associated with development of post-traumatic epilepsy (PTE)) as well as overall morbidity and mortality in TBI patients. Based on the American Academy of Neurology (AAN) and Brain Trauma Foundation (BTF) recommendations, using anti-seizure drugs during the first seven days after an injury has become the standard of care for PTS prophylaxis in severe TBI patients.
The two most commonly used anti-epileptic drugs are fosphenytoin (Dilantin)/phenytoin (Cerebyx) and levetiracetam (Keppra). A recent systematic review and meta-analysis showed no significant difference between the two in reducing early or late-onset PTS.10 The use of levetiracetam for post-traumatic seizure prophylaxis is somewhat more common, presumably due to the ease of dosing, fewer interactions with other drugs, and lack of need for frequent blood level monitoring. For additional information regarding comparison of fosphenytoin (Dilantin)/phenytoin (Cerebyx) and levetiracetam (Keppra), please refer to Appendix A.
Anti-Epileptic Drugs and Doses
- Phenytoin (Dilantin)/Fosphenytoin (Cerebyx):
- Loading dose: fosphenytoin 15mg/kg (rounded to nearest 50mg)
- Administered over 150mg/min (e.g. 1g load given over 7 minutes)
- Maintenance dose:
Weight Phenytoin Phenytoin extended release <80 kg 100mg PO/IV q 8 hours 300mg PO qHS 80 – 110 kg 150mg PO/IV q 8 hours 400mg PO qHS >110 kg Consult pharmacy Consult pharmacy - Enteral tube feeds impair the absorption of phenytoin capsules by up to 70%, so tube feeds should be held for 2 hours before and after administration.
- Extended release phenytoin should not be crushed and put down an enteral feeding tube as this may affect the extended release properties.
- Levetiracetam (Keppra):
- Loading dose: 1g IV once
- Maintenance dose: 1g PO/IV q12 hours x 7 days post-injury
- Pills can be crushed and put down enteral feeding tubes without tube feed disruption.
APPENDIX A
Despite the increasing use of levetiracetam, there has been no large, prospective, randomized controlled trial comparing the effectiveness of levetiracetam to phenytoin though there have been prospective observational and small randomized clinical trials.
Below are the results of a limited search for studies comparing phenytoin and levetiracetam including: randomized clinical trials, prospective observational studies, and prospective observational studies using a historical control group. The search was limited as there are a number of systematic reviews published within the past decade, which were used to ensure no relevant study was missed.
| Author/Year | Study Type | Patients, n | Inclusion Criteria | Exclusion Criteria | Dosage | Outcomes |
|---|---|---|---|---|---|---|
| Szaflarski, 20101 | RCT (2:1 LEV to PHE) | 52 (18 PHE, 34 LEV) | Severe TBI, SBP >90 mmHg, Age ≥17 years | No venous access, SCI, history of TBI, hemodynamic instability, anoxic injury, liver failure | PHE: 20mg/kg fos-PHE load, then 5mg/kg/day divided q12 hours (levels followed) LEV: 20mg/kg IV load, then 1g IV q12 hours |
Early Post-Traumatic Seizures PHE – 5/18 (17%) LEV – 7/34 (15%) |
| Note: in the above study, all patients were monitored with continuous EEG for 72 hours or until awake and following commands to identify subclinical seizures. | ||||||
| Khan, 2016 2 | RCT (1:1 LEV to PHE) | 154 (77 PHE, 77 LEV) | Moderate or severe TBI and age 5-50 years | History of prior sz, delayed presentation >12h, renal or electrolyte derangements, pts undergoing surgery, pts who died within 7d | PHE: 20 mg/kg PHE load, then 5 mg/kg/d divided Q12H (serum levels not measured) LEV: 20 mg/kg LEV load, then 10-20 mg/kg divided Q12H |
Early Post-Traumatic Seizures PHE – 4/77 (5.2%) LEV – 7/77 (7.1%) |
| Note: the above study is at moderate to high risk for bias due to absence of PHE serum level monitoring, absence of continuous EEG, lack of blinding, and unclear randomization/allocation technique | ||||||
| Inaba, 2013 3 | Prospective observational | 813 (407 PHE, 406 LEV) | Blunt TBI Age ≥18 years |
Pregnancy, non-survivable TBI, prehospital AED use, seizure before enrollment | PHE: 20mg/kg IV load, then 5mg/kg/day divided q8 hours (levels followed) LEV: 1g IV q12 hours |
Early Post-Traumatic Seizures PHE – 6/407 (1.5%) LEV – 6/406 (1.5%) |
| Note: in the above two center study, the majority of PHE patients were clustered at one center (396/407) and the majority of LEV patients were clustered at the other (329/406). | ||||||
| Jones, 2008 4 | Prospective observational (LEV) compared to historical control (PHE) | 73 (PHE 41, 32 LEV) | Severe TBI | Not stated | PHE: unclear LEV: 500mg IV q12 hours |
Early Post-Traumatic Seizures PHE – 0/41 (0%) LEV – 1/32 (3%) Abnormal EEG Findings PHE – 0/32 (0%) LEV – 8/42 (19%) |
| Note: in the above study, EEG were performed as needed – 15/32 LEV patients underwent 19 EEG and 12/41 PHE patients underwent 19 EEGs. | ||||||
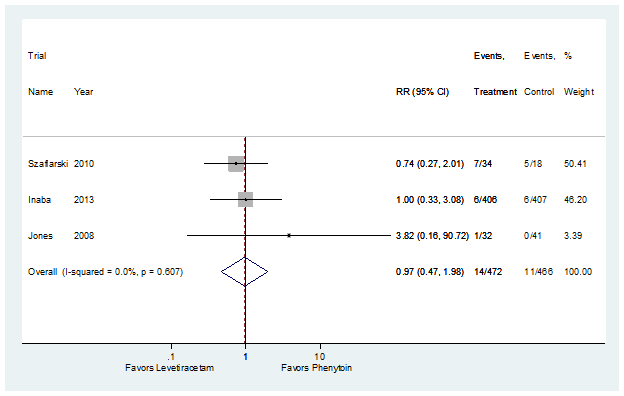
Forest plot of three included studies for the outcome: early post-traumatic seizures.
Cost Considerations:
Multiple studies have addressed the issue of cost associated with levetiracetam. , However, there has recently been a reduction in the cost of levetiracetam have alleviated. The overall cost of multiple treatment strategies are delineated below:
| Treatment Strategy |
Load | Maintenance | Total Cost |
|---|---|---|---|
| 1 | 1g fosphenytoin | phenytoin 100mg IV q8° x 7 days | $X |
| 2 | 1g levetiracetam | levetiracetam 1g IV q12 x 7 days | $0.95X |
| 3 | 1g levetiracetam | levetiracetam 1g IV q12 x 3 days levetiracetam 1g PO tab q12 x 4 days |
$0.77X |
| 4 | 1g levetiracetam | levetiracetam 1g IV q12 x 3 days levetiracetam 1g PO suspension q12 x 4 days |
$1.10X |
| 5 | 1g phenytoin | phenytoin 100mg IV q8° x 7 days | $0.22X |
Actual costs cannot be displayed. However, the costs of different regimens are provided in the form of multiples of the cost of fosphenytoin load followed by 7 days of IV phenytoin.
As there are a number of recent systematic reviews regarding this topic, a more limited search was performed and the multiple systematic reviews were used to ensure that no relevant article was missed. Search limitations included: English language, randomized clinical trial, and prospective observational study (with or without historical control).
| Search | Database | Search Term | Limits | Total Yield: # of Articles | # Excluded Articles | # Included Articles |
|---|---|---|---|---|---|---|
| 1 | PubMed | phenytoin AND levetiracetam AND traumatic brain injury | Clinical Trial | 4 | 1 (LEV not compared to PHE) | 1 Prospective observational, 2 RCT |
| 2 | PubMed | phenytoin AND levetiracetam AND traumatic brain injury | Randomized Controlled Trial | 3 | 0 | 1 Prospective observational, 2 RCT (all duplicates) |
| 3 | PubMed | phenytoin AND levetiracetam AND traumatic brain injury | Systematic Review | 9 | 1 (outcome late post-traumatic seizure); 1 (LEV compared to placebo or no Tx); | 7 |
| TOTAL | 16 | 3 | 10 | |||
| Exclude Multiples 3 | ||||||
| Included Papers 10 (2 RCTs, 1 Observational, 7 SRs) | ||||||
Systematic Reviews evaluated:
- Khan NR, et al. Should Levetiracetam or Phenytoin Be Used for Posttraumatic Seizure Prophylaxis? A Systematic Review of the Literature and Meta-analysis. Dec 2016;79(6):775-82
- Yang Y, et al. Levetiracetam Versus Phenytoin for Seizure Prophylaxis Following Traumatic Brain Injury: A Systematic Review and Meta-Analysis. CNS Drugs. Aug 2016;30(8):677-88
- Xu JC, et al. The Safety and Efficacy of Levetiracetam Versus Phenytoin for Seizure Prophylaxis after Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Brain Inj. 2016;30(9):1054-61
- Thompson K, et al. Pharmacological Treatments for Preventing Epilepsy Following Traumatic Head Injury. Cochrane Database Syst Rev. Aug 2015;(8):CD009900
- Zafar SN, et al. Phenytoinversus Levetiracetam for Seizure Prophylaxis after Brain Injury – a meta analysis. BMC Neurol. May 2012;12:30
- Wilson CD, Burks JD, Rodgers RB, Evans RM, Bakare AA, Safavi-Abbasi S. Early and Late Posttraumatic Epilepsy in the Setting of Traumatic Brain Injury: A Meta-analysis and Review of Antiepileptic Management. World Neurosurg. 2018 Feb;110:e901-e906. doi: 10.1016/j.wneu.2017.11.116. Epub 2017 Dec 2. PMID: 29196247.
- Zhao L, Wu YP, Qi JL, Liu YQ, Zhang K, Li WL. Efficacy of levetiracetam compared with phenytoin in prevention of seizures in brain injured patients: A meta-analysis. Medicine (Baltimore). 2018 Nov;97(48):e13247. doi: 10.1097/MD.0000000000013247. PMID: 30508910; PMCID: PMC6283080.
- Timothy A. Amin, Steven F. Nerenberg, Osama A. Elsawy, Antai Wang, Jackie P. Johnston
Review of the systematic reviews failed to identify a missed randomized clinical trial, prospective observational study, or prospective observational study using a historical control.
- Szaflarski JP, et al. Prospective, Randomized Single-Blinded Comparative Trial of Intravenous Levetiracetam Versus Phenytoin for Seizure Prophylaxis. Neurocrit Care. Apr 2010;12(2):165-72.
- Khan SA, Bhatti SN, Khan AA, Khan Afridi EA, Muhammad G, Gul N, Zadran KK, Alam S, Aurangzeb A. Comparison Of Efficacy Of Phenytoin And Levetiracetam For Prevention Of Early Post Traumatic Seizures. J Ayub Med Coll Abbottabad. 2016 Jul-Sep;28(3):455-460. PMID: 28712212.
- Inaba K, et al. A Prospective Multicenter Comparison of Levetiracetam versus Phenytoin for Early Post-Traumatic Seizure Prophylaxis. J Trauma Acute Care Surg. Mar 2013;74(3):766-71.
- Jones KE, et al. Levetiracetam Versus Phenytoin for Seizure Prophylaxis in Severe Traumatic Brain Injury. Neurosurg Focus. Oct 2008;25(4):E3
- Cotton BA, et al. Cost-Utility Analysis of Levetiracetam and Phenytoin for Post-Traumatic Seizure Prophylaxis. J Trauma. Aug 2011;71(2):375-9
- Pieracci FM, et al. A Cost-Minimization Analysis of Phenytoin Versus Levetiracetam for Early Seizure Pharmacoprophylaxis after Traumatic Brain Injury. J Trauma Acute Care Surge. Jan 2012;72(1):276-81
- Evaluation of levetiracetam for early post-traumatic seizure prophylaxis: A level II trauma center experience, The Surgeon, volume 21, issue 2, 2023, pages e78-e82, ISSN 1479-666X, https://doi.org/10.1016/j.surge.2022.05.001.
- Karamian A, Farzaneh H, Taheri M, Seifi A. Effectiveness of Levetiracetam versus phenytoin in preventing seizure in traumatic brain injury patients: A systematic review and meta-analysis. Clin Neurol Neurosurg. 2024 May;240:108251. doi: 10.1016/j.clineuro.2024.108251. Epub 2024 Mar 20. PMID: 38569246.