ICU Palliative Care
Original Date: 12/2021 | Last Reviewed Date: 12/2024
Purpose: To standardize the consultation of the Supportive Medicine team.
The Supportive Medicine team is available to:
- Assist with goals of care conversations
- Assist with symptom management
- Provide support for families including child life services
- Provide support the team/staff
- Assume care of patients when appropriate
Supportive Medicine consultation should be obtained on hospital day 1 for a patient:
- Whom the Burn Surgeon has determined to have a fatal burn injury and no operative management is planned.
- With a Grade 4 inhalational injury.
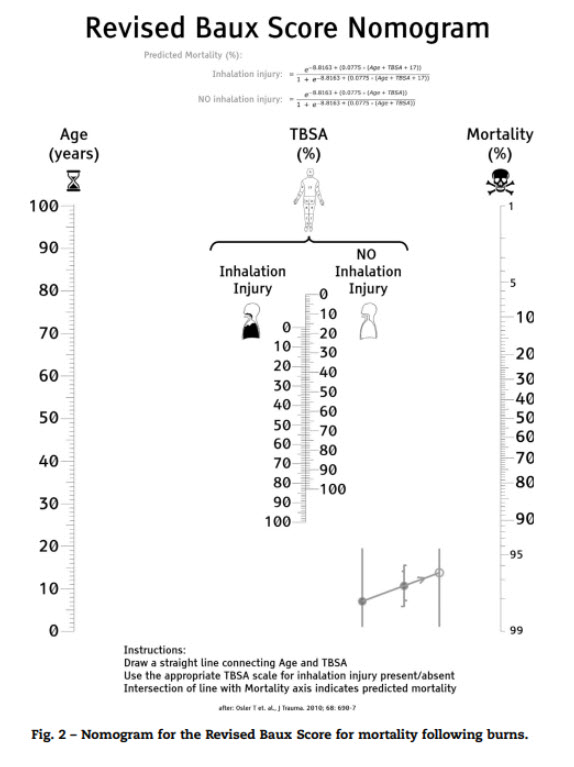
- With a revised Baux score >140.
- With a life limiting medical condition and ≥20% TBSA burn.
- Who presents from hospice care.
Supportive Medicine consultation should be obtained by hospital day 3 on patients:
- Over 65 years of age with a ≥20% TBSA burn who develop an organ failure during resuscitation.
- Examples:
- Kidney failure requiring hemodialysis
- Respiratory failure requiring new or ongoing mechanical ventilation
- New onset heart failure requiring inotropic support
- Any patient requiring vasopressor support
- Over 65 years old with who is likely to lose functional independence at time of discharge.
- Example:
- Including burn injury requiring amputation
- With a revised Baux Score >125.
- Example:
- Examples:
Family meetings should include:
- Burn ICU attending and/or Burn surgeon
- Burn intern or PA
- Supportive Medicine consultant
- Burn bedside and/or charge nurse
Supportive care agreement:
- Team is on campus 9 am – 4 pm on weekdays, and 9 am – Noon on weekends/holidays/skeleton crew days
- To consult: place an order in EPIC for “Inpatient consult to Supportive Medicine”
- Contact Supportive Medicine: send chat message through EPIC to either “supportive medicine weekday” or “supportive medicine weekend”
- If the Supportive Medicine team takes over a patient for comfort care, keep the patient on the list in case death occurs while the team is not here then: pronounce patient dead, call the family, and call the ME if needed. You don’t have to see or round on the patient after Supportive Medicine takes over and they will still take care of the discharge summary even if the burn service pronounces the patient.
If patient transitions to Hospice, the Supportive Medicine team will take over as primary team. The Burn Service should continue to be aware of the patient and remain on burn list. If the patients passes overnight or on the weekend, the Burn Service declares the patient, notifies the medical examiner, and notifies the Supportive Medicine team.