Pediatric Venous Thromboembolism (VTE) Guideline & Algorithm
Original Date: 11/2011 | Supersedes: 08/2016, 06/2017, 10/2020 | Last Review Date: 10/2023
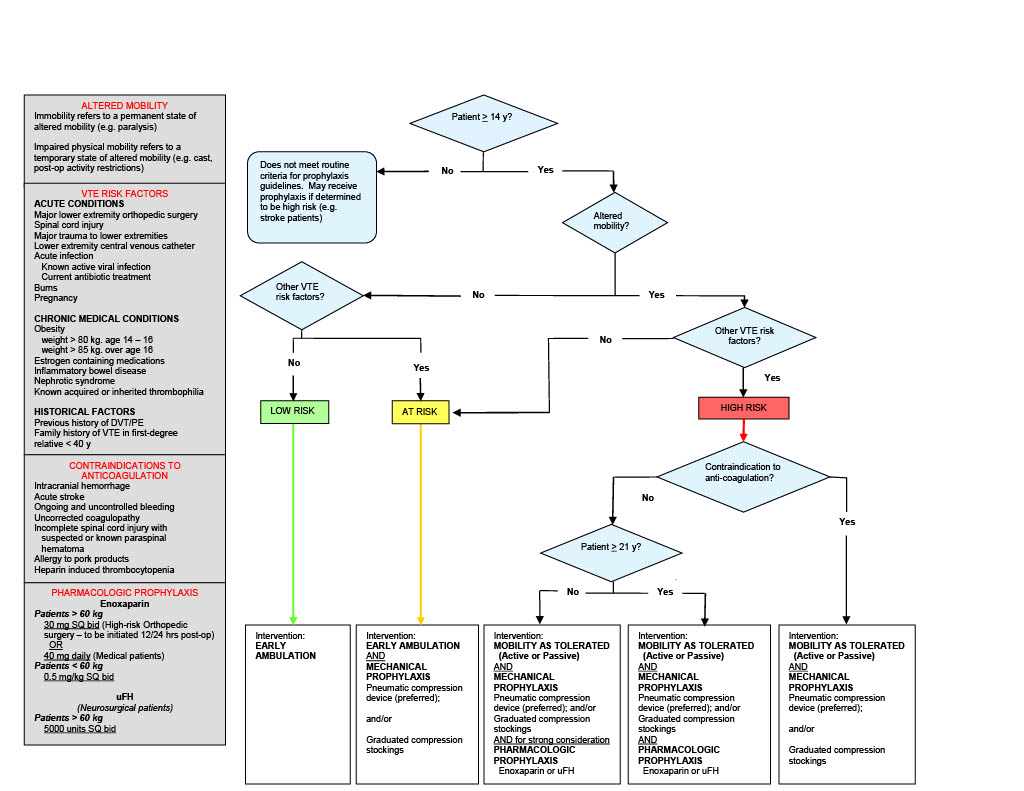
Purpose: To define pediatric patient populations at risk for VTE and their prophylaxis.
Procedure
For patients at high risk of VTE1 with low risk of bleeding2:
- anticoagulate with low molecular weight heparin at 0.5mg/kg subcutaneous, twice daily until hospital discharge
For patients at high risk of VTE1 with high risk of bleeding3:
- apply sequential compression devices
- on PICU day 7 obtain screening ultrasound of bilateral lower extremities, and upper extremity if CVL is present
For patients at low risk of VTE4:
- no anticoagulation or other clinical intervention indicated
Risk Factors for VTE:
- projected immobility > 5 days
- Glasgow Coma Scale less than 9
- presence of CVL
- spinal cord injury
- complex lower extremity fracture
- operative pelvic fracture
- use of inotropes
- CPR during resuscitation
- exogenous estrogen
- chronic inflammatory state
- history of previous clot
- known thrombophilia
- current malignancy
Risk Factors for Bleeding:
- intracranial bleed
- solid organ injury
- planned surgical intervention or invasive procedure in the next 24 hours
- heparin allergy
- high risk of severe bleeding
- renal failure
1High risk of VTE defined as age greater than 13 years OR age less than 13 years with four or more risk factors for VTE.
2Low risk of bleeding defined as no risk factors for bleeding.
3High risk of bleeding defined as one or more risk factors for bleeding.
4Low risk of VTE defined as age less than 13 years AND three or fewer risk factors for VTE.
VTE = venous thromboembolism; PICU = pediatric intensive care unit; CVL = central venous line; CPR = cardiopulmonary resuscitation
References:
Carrillo, L., Kumar, A., Harting, M., Pedroza, P., Cox, C. (2019). Venous thromboembolism risk factors in a pediatric trauma population. Pediatric Surg Int, 35(4), 487-493. doi: 10.1007/s00383-018-4418-y
Landisch RM, et al. (2017). Evaluation of guidelines for injured children at high risk for venous thromboembolism: A prospective observational study. J Trauma Acute Care Sur, 82, 836-844.
Liras IN, et al., (2016). When children become adults and adults become most hypercoaguable after trauma: An assessment of admission hypercoaguability by rTEG and venous thromboembolic risk. J Trauma Acute Care Surg, 80, 778-782.