UT Health/CMHH modified ATOMAC guideline for management of pediatric BLSI
Original Date: 06/2017 | Supersedes: 09/2021 | Last Review Date: 03/2024
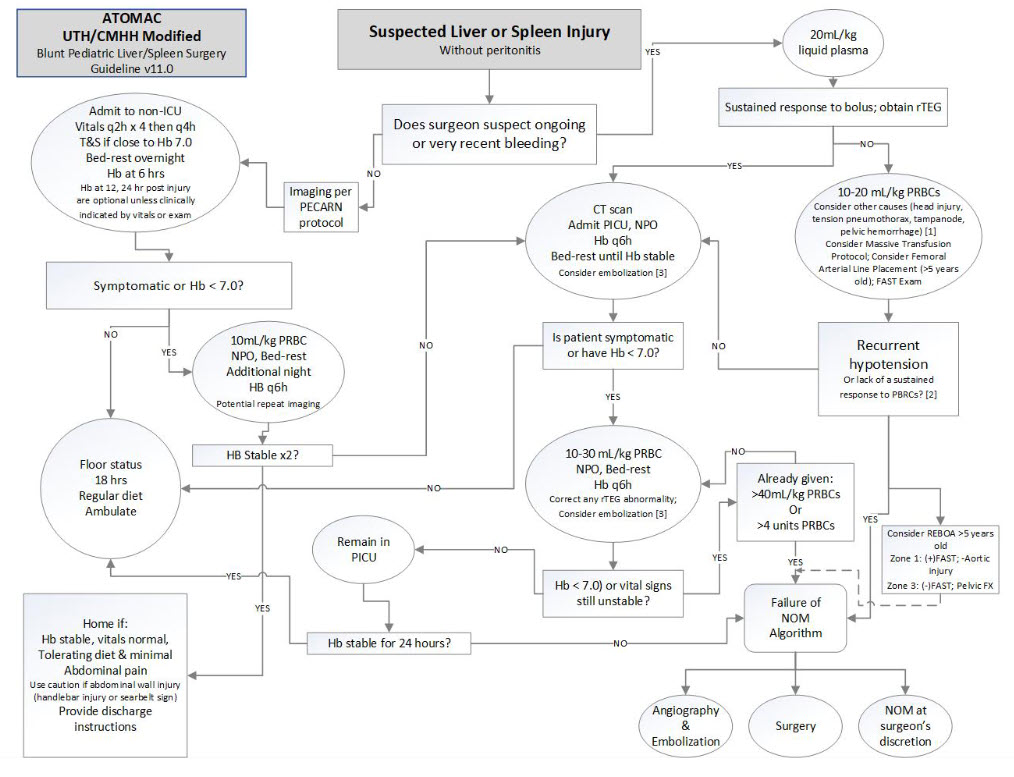
Figure 1. UT Health/CMHH modified ATOMAC guideline for management of pediatric BLSI. 1More than 50% of injured children with hypotension have no significant intra-abdominal bleeding but do have severe traumatic brain injury. 2Recurrent hypotension within the first hour because of intra-abdominal bleeding or an SBP of less than 50 mm Hg after transfusion is an ominous sign, and strong consideration should be given to operative or angiographic intervention. 3Embolizing CT blush may be considered, but more than 80% of children with blush do not require angiography for successful NOM. 4Interventional modalities such as ERCP, laparoscopy, angiography, or percutaneous drainage may be required to manage complications of bile leak or hemobilia. Hb, hemoglobin; NPO, ‘‘non per os’’ or nothing per mouth; PICU, pediatric ICU; PRBC, packed red blood cell; q6h, every 6 hours; SBP, systolic blood pressure.
REBOA = Resuscitative endovascular balloon occlusion of the aorta. REBOA balloon volumes: Zone 1; 5-10 years old 3-4ml; 10-15 years old 4-6ml. Zone 3; 5-10 years old 2-3ml; 10-15 years old 4-6ml.
Notrica DM, Eubanks JW, Tuggle DW, et al., Nonoperative management of blunt liver and spleen injury in children: Evaluation of ATOMAC guideline using GRADE. J
Trauma Acute Care Surg 79: 683-693, 2015.