Interprofessional Consultation
What it is
Interprofessional consultation codes describe non–face-to-face, provider-to-provider consultative services in which a treating/referring provider requests the medical opinion or treatment advice of a consulting physician or other qualified healthcare professional without the consultant seeing the patient.
What it isn’t
These codes are not telehealth, not curbside teaching, and not resident supervision.
CPT Codes
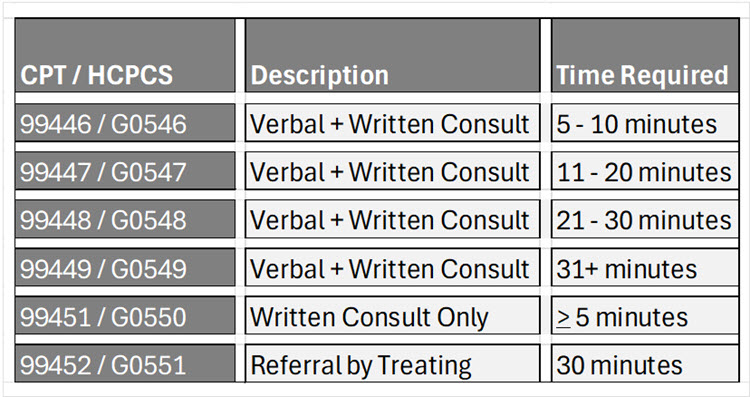
- Time is cumulative and includes record review + consultative discussion
- >50% of time must be medical consultative discussion for 99446–99448
- Only consulting provider time counts
- Medicare G-codes are for use by Behavioral Health providers only
Documentation Requirements
Must meet all:
- Consult request from treating/referring provider
- No face-to-face encounter by the treating/referring provider
- No visit in prior 14 days
- No planned visit in next 14 days
- Only report ONCE per 7 days
- Consultative service provided for patient care
- Not education, supervision, or professional courtesy
- Verbal discussion + written report (99446-99448)
- Written report only (99451)
- Time – >50% of time must be medical consultative discussion
- Patient consent obtained by referring/treating provider
Compliance tip: When an Attending Involves Residents, Fellows, or APPs
If any trainee or APP sees the patient face-to-face, the service NO LONGER qualifies as an interprofessional consultation.
Trainees
• Under CMS teaching physician rules, resident/fellow services are attributed to the attending
• A face-to-face specialty service has occurred
• Interprofessional consultation codes are explicitly prohibited in this situation
Bottom line:
If a resident, fellow, or APP evaluates the patient → DO NOT use 99446–99451 Use the appropriate face-to-face E/M consult or inpatient visit rules instead.
Sample Documentation Statement
Interprofessional Consultation Note
I received a request from [requesting provider name, credentials] for interprofessional consultation regarding [brief patient problem].I did not have a face-to-face encounter with the patient and have not seen the patient within the prior 14 days, nor is a face-to-face visit planned within the next 14 days.
I reviewed the relevant clinical information and engaged in direct medical consultative discussion with the requesting provider. A written report of my assessment and recommendations was provided.Total interprofessional consultative time personally spent by me: [XX] minutes, with greater than 50% devoted to medical consultative discussion.
Patient consent for interprofessional consultation was obtained and documented by the requesting provider.
Final Take Aways
Interprofessional consultation codes (CPT® 99446–99452) were created to formally recognize and reimburse provider‑to‑provider cognitive work performed for the direct benefit of the patient. However, these codes exist within a narrow and carefully defined compliance framework.
Key points to remember:
- Only patient‑specific consults are billable.
Informal discussions, curbside teaching, and supervisory interactions do not qualify as interprofessional consultations. - Who performs the work matters.
If a trainee sees the patient, interprofessional consultation codes cannot be used. Only the consulting attending’s personally performed time may be counted. - Clear documentation reduces audit risk.
Notes must show a requested, patient‑specific consult, attending‑only time, and acknowledgment of patient consent. Templated or vague language increases risk.
Resources
Novitas – G0556 – G0552
AAPC – CPT Assistant Summary
CodingIntel Article – Interprofessional Internet Consultations
CMS Pub 100‑04, Chapter 12 – Teaching Physician Services
42 CFR §415 Subpart D – Physician Services in Teaching Settings