Repair of DeBakey Type I Acute Aortic Dissection, by Tanaka & Estrera
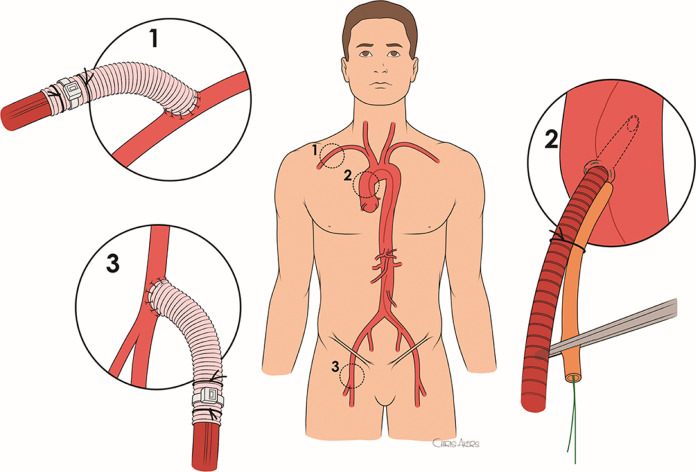
Figure 1. Cannulation sites. (1) Axillary cannulation with an 8-mm Dacron graft anastomosed to the artery in end-to-side fashion with a running 5-0 polypropylene suture. The graft is beveled in a fashion to flow more toward central rather than distally to the arm. (2) Direct ascending aortic cannulation.
Full article available online and in the February 2021 print edition of Operative Techniques in Thoracic and Cardiovascular Surgery: A Comparative Atlas: A Comparative Atlas provides technique-based articles in cardiovascular and thoracic surgery by renowned surgeons in the field, presented in atlas format.
Written by fourth year integrated vascular surgery resident, Akiko Tanaka, MD, PhD, and chair and professor of cardiothoracic and vascular surgery at McGovern Medical School at UTHealth, Anthony Estrera, MD.
“Acute DeBakey type I aortic dissection remains one of the most lethal cardiovascular emergencies. Surgical mortality after acute aortic dissection repair are 17-18%—and the extent of repair has been controversial. Herein, we describe our current “tear-oriented” approach to treat DeBakey type I aortic dissection. We believe the surgical techniques selected should be based on each surgeon’s experience, focusing on minimizing the complexity of the procedure and reducing surgical morbidity and mortality rather than preventing future operations.”